






80% of all your future revenue will come from just 20% of your existing customers
Source: Gartner
Building long-term value
A sale is only the beginning of the customer journey. The teams responsible for guiding relationships through each stage of the customer lifecycle build lasting value for your business.
Synap is designed for post-sales engagement, helping teams to build, collaborate, and execute their plans to grow customer relationships.
Tools to build relationships
-
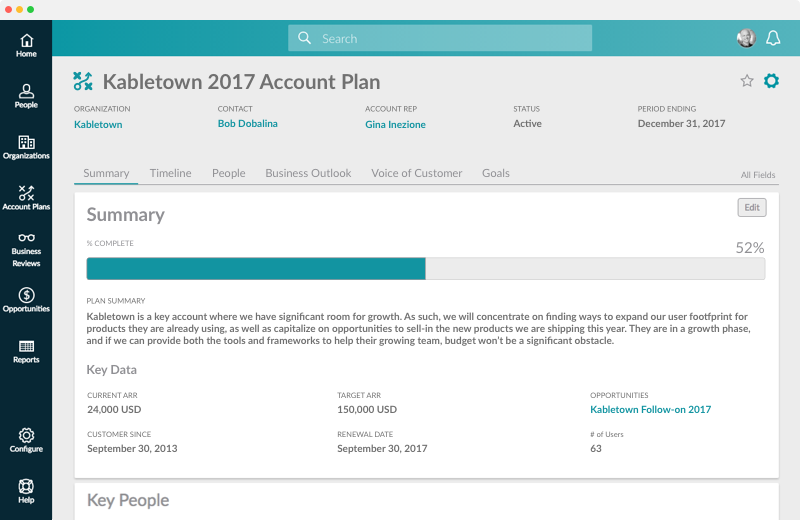
Account Planning
Get strategic about account growth. Map the important players, identify opportunites, and set goals for your key accounts.
-
Shared Communications
Track everyone’s customer activities in one place. Emails, support tickets, and notes are all automatically added to customer records.
-
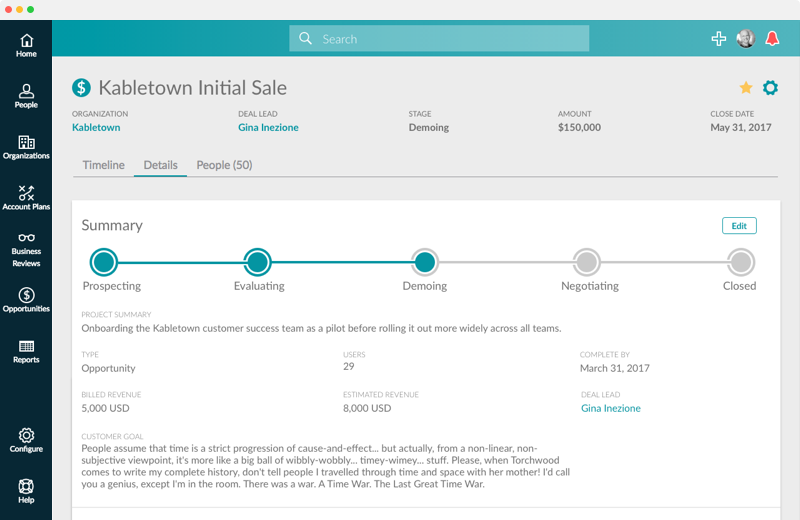
Opportunity Management
Identify upsell opportunities. Coordinate sales, success, and services to execute customer-centric sales cases.
Our customer onboardings are very high-touch and require us to respond quickly. Synap makes perfect sense for us during this critical phase of our customer engagements.


Lou Jacob
VP of Customer Success